RENAL TRAUMA
Kidney damage is a major concern in any abdominal trauma.
In fact,
about 10% of abdominal traumas result in some extent of renal injury,
even though majority of lesions will be minor.
Ultrasound might be the first approach in several centers due to its non-invasiveness,
portability and promptness to be used in the emergency department.
Nevertheless,
contrast-enhanced CT is the modality of choice in the evaluation of renal trauma due to its accuracy in the detection of this and other abdominal/retroperitoneal injuries,
active hemorrhage and urine leakage.
Moreover,
it has an increasing role in embolization planning,
with angiography growing now as a therapeutic modality.
I – MECHANISM OF INJURY
About 80 to 90 % of renal trauma is due to blunt abdominal trauma,
resulting from rapid deceleration or crush injuries.
Among these,
motor vehicle accidents are the most important cause.
Nevertheless,
falls from height and sports activities,
like horseback riding are also causes to consider.
Penetrating trauma is less common,
representing only 10 to 20% of renal injuries.
The damage is caused by direct damage to the parenchyma,
excretory or vascular structures.
There is increased risk of infection due to the existence of an entry port.
Gunshot or stab wounds are the most common.
Nonetheless,
the incidence of iatrogenic injuries has risen,
especially with the increasing number of renal biopsies performed.
II –IMAGING STUDIES AND INDICATIONS
Evaluation of the patient with trauma using ultrasound,
particularly with the FAST protocol,
has the primary goal of identifying intraabominal free fluid.
Detection of fluid in the hemodinamically unstable patient is considered to represent hemoperitoneum and warrants immediate surgery.
Hemodinamically stable patients with free fluid detected or nonconclusive ultrasound should undergo a CT examination.
The same patients can be followed clinically (not needing a surgical approach) if the ultrasound does not reveal free fluid.
Angiography has a decreasing role as a diagnostic tool due to the greater accuracy of CT.
Most commonly,
it is nowadays performed for selective or supraselective embolization of renal arteries.
III - AAST GRADING SYSTEM
Despite the several classification systems developed,
the American Association for the Surgery of Trauma (AAST) is the most used one.
It is based on surgical findings and correlates well with prognosis,
but also with CT abnormalities.
It divides renal injuries into five categories (grades I – V),
with increasing severity (Figure 1).
Bilateral lesions will have one grade upgrade.
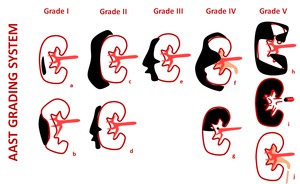
Fig. 1: AAST Grading system for renal trauma.
Grade I: Renal contusion (a) and subcapsular hematoma without laceration(b); Grade II: Perinephric hematoma within the retroperitoneum (c) and small laceration less than 1 cm in depth (d); Grade III: Lacerations greater than 1 cm but without collecting system involvement (e); Grade IV: Renal laceration extending to the medulla and collecting system (f) and segmental infarctions without laceration (g). Injuries of the renal artery or vein with contained hematoma are also included in this category. Grade V: Shattered kidney (h), thrombosis of the renal artery or vein that devascularizes the kidney (i) and ureteropelvic junction avulsion (j).
Bilateral injuries will have one grade upgrade.
III.I.
Grade I Injuries
Grade I lesions are the most frequently seen (75-85% of cases) and less severe injuries.
In this category are included contusions as well as subcapsular hematomas without laceration.
Contusion represents an intra-parechymal hematoma.
On CT it is seen as a focal areas of decreased contrast enhancement within the kidney,
frequently ill-defined,
with a round or oval shape.
It may also appear as an area of focal delayed nephrogram and tens to be hypoattenuating unless it is filled with clots,
in which case it will show as spontaneously hyperratenuating non-enhancing area (Figure 2).
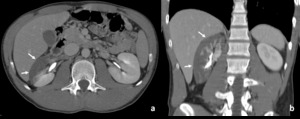
Fig. 2: Patient with renal contusion (AAST grade I).
CT in a patient reporting blunt trauma demonstrating lack of renal enhancement with irregular border in more than 50% of the right kidney (arrows in a and b). Absence of enhancement is noted in the anterior and peripheral parenchyma. The kidney still mantains its normal contour. These abnormalities are consistent with contusion.
Subcapsular hematomas accumulate eccentrically between the parenchyma and the renal capsule.
Their imaging appearance varies with acuteness between spontaneous heterogenous hyperattenuating collections to homogeneous,
iso or hypoattenuating collections after several days to weeks.
They do not reveal contrast enhancement and for this reason it is fundamental to perform an acquisition before contrast administration.
Small hematomas tend to be crescent shaped,
but with bigger volumes they tend to compress the renal parenchyma and deform its margins (Figure 3).
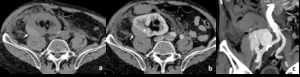
Fig. 3: Patient with subcapsular hematoma in a transplanted kidney (Grade I AAST).
CT in a transplanted kidney patient reporting blunt trauma demonstrating hypeattenuating subcapsular collections in the transplanted kidney, located in the right iliac fossa (arrows in a and b). Contrast-enhancement allows to confirm the presence of a renal collecting compressing the parenchymal contour (arrowhead in b), consistent with subcapsular hematoma.
III.II.
Grade II Injuries
If the capsule is lacerated after a renal trauma,
the blood may extend from a subcapsular location to the perinephric space,
delimited between the anterior renal fascia of Gerota and the posterior renal fascia of Zuckerkandl.
If the hematoma remains in the retroperitoneal space,
it is considered grade II.
With extension in the retroperitoneum,
thickening of the lateroconal fascia and displacement of other organs as the head of the pancreas,
duodenum or colon might be seen.
Despite this,
it is less common for a perinephric hematoma to exert mass effect on the kidney,
changing its shape,
than it is for the subcapsular hematoma.
Also small lacerations,
not exceeding 1 cm in parenchymal depth are in this category.
They are seen in imaging as an irregular,
sometimes wedge shaped,
parenchyma enhancing defect.
They may show hyperattenuation if filled with clots,
but shouldn't have contrast enhancement.
Unlike renal infarcts,
they tend to have irregular margins (Figure 4).
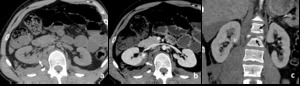
Fig. 4: Renal laceration inferior to 1 cm (AAST grade II).
CT in a patient reporting blunt trauma revealing irregularity of the posterior right renal contour with densification (arrow in a). After contrast enhacement an hematoma envolving the posterior border of the kidney can be seen (arrow in b), along with irregularity of the parenchyma, representing small laceration, inferior to 1 cm in depth (arrowhead in b). The laceration can also be seen adjacent to the hilum in the coronal reformatation(arrowhead in c). Fractures of two vertebra are also demonstrated, findings than commonly occur with these injuries (black arrows in c).
Any Grade I injury will be upgraded to Grade II if it is bilateral (Figure 5).

Fig. 5: Bilateral subcapsular hematoma (Grade II AAST injury).
CT in a patient reporting blunt trauma demonstrating hyperattenuating subcapsular collections in both kidneys, previously to contrast administration (white arrows in a). Contrast-enhancement allows to confirm absence of renal laceration. The renal contour is better appreciated in this image and shows bilaterally to be distorted by these collections (black arrows in b) that are well limited peripherally, where they contact the capsule, so one can assume to be a bilateral subcapsular hematomas. In fact, they do not contact renal fasciae (arrowheads in b showing the anterior renal fascia). The same abnormalities can be seen in the coronal image, obtained during the excretory phase, showing no involvement of the collecting system of the right kidney (asterisk in c).
This patient would be categorized as having a grade I renal injury due to subcapsular hematoma, but because of being injury, it increases one grade, being classified as grade II injury.
III.III.
Grade III Injuries
Grade III injuries also represent renal lacerations,
but ones that have more than 1cm of depth.
Still,
Grade III lesions should not demostrate collecting system injury (Figure 6).
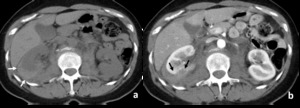
Fig. 6: Renal laceration deeper than 1 cm (AAST grade III).
Patient with blunt trauma in which non-enhancing CT reveals the presence of a hyperdense collection consistent with hematoma (arrows in a). The renal contour is well defined and does no appear to be distorted, suggesting hematoma in the peri-nephric space and not subcapsular hematoma. Contrast-enhanced CT reveals laceration in the posterior pole of the right kidney extending for more than 1 cm (arrows in b). Capsular rupture explains why the blood extends to the perirenal space.
III.IV.
Grade IV Injuries
Lacerations exteding to the collecting system,
injuries of the renal main vessels with hemorrhage or segmental infarctions without lacerations are the hallmark of grade IV.
When lacerations affect the renal collecting system,
urine escapes to the retroperitoneum,
which can be demonstrated in the delayed excretory phases of CT (Figure 7).

Fig. 7: Patient with a renal laceration exteding to the collecting system (Grade IV AAST). Patient with blunt trauma in which non-enhancing CT demonstrates an hyperdense collection involving the right kidney, correponding to a perirenal hematoma (arrows in a). Contrast-enhaced aquisition also reveals a deep laceration in the same kidney, extending to the renal medulla (asterisk in b). Excretory phase aquisition (5 min after contrast administration) allows the detection of urine extravasion from the renal calyx (arrowhead in c) to the collection involving the kidney (arrows in c and d).
Infarctions are seen as nonenhancing areas with regular borders and a wedge shape,
having a peripheral base and a center directed to the hilum.
The absence of parenchymal laceration in these cases suggests a vascular process,
such as thrombosis,
dissection or laceration of the artery.
The size of the affected vessels correlates with the dimension of the nonenhancing area.
III.V.
Grade V Injuries
In the most severe category of renal injuries are shattered kidneys,
lesions with avulsion of the ureteropelvic junction and thrombosis of the major renal vessels with devascularization of the kidney.
Shattered kidney is the most severe form of renal laceration,
resulting in a kidney with multiple fragments.
Devitalized areas may appear,
but can be underappreciated when surrounding hematoma is present.
Injuries of the collecting system and active bleeding are common (Figure 8).
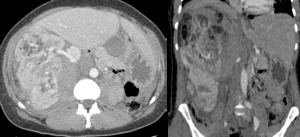
Fig. 8: Shattered kidney (Grade V AAST).
Patient with major blunt trauma on the right flank and hematuria showing multiple lacerations of the right kidney, making its contours difficult to distinguish (a and b). These fragments still show normal enhancement, revealing maintained perfusion.
Ureteropelvic junction injuries may result from deceleration.
Hematuria may nevertheless be absent in one third of cases.
Partial tears are seen if the urine extravasion appears with distal ureteric contrast opacification.
If distal opacification is not seen,
the tear is considered to be complete.
Among vascular pathologies,
renal artery occlusion is the most common event.
With an injury of the artery,
intimal tear or dissection might activate the coagulation cascade which might lead to thrombus being formed.
The occlusion will lead to absence of vascularity of a renal segment,
which will not show enhancement on CT (Figure 9).
Still,
a small capsular enhancement can be seen if collateral capsular vessels are preserved.
It requires at least eight hours of evolution of infarct,
which explains is not to so commonly identified in the acute patient.
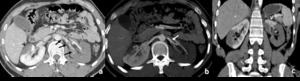
Fig. 9: Bilateral renal infactions secondary to thrombosis.
Contrast-enhanced CT shows multiple thrombi in the left renal artery, two more proximally that occlude the renal artery partially and multiple distally, occluding the major branch (black arrows in a). A segmental infarction is also seen in the left kidney (arrowhead in a), which shows the classic triangular shape of a non-enhancing renal area, maintaining the normal renal contours. MIP reformatation depicts the branching of the left renal artery at the renal hilum, giving an anterior branch which supplies the only vascularized area of this kidney (arrowhead in c), and a posterior branch that shows complete occlusion.
Renal vein thrombosis can be seen,
but usually is identified along with arterial or parenchimal pathology.
CT may show venous engorgement and the thrombus can be visualized.
Renal vein laceration might be difficult to depict,
but should be suspected when subcapsular or perinephric subcapsular hematoma is found.
IV – Active bleeding
Active bleeding is not included in the AAST,
which is based on surgical findings primarily.
It may appear on contrast-enhanced CT as linear or irregular images of high attenuation outside the vessels.
The extravasion point should try to be detected in order to guide the angiographic or surgical intervention (Figure 10).
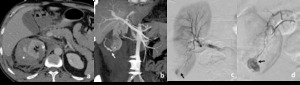
Fig. 10: Patient with renal laceration and active bleeding.
Contrast enhanced CT in a patient with trauma showing right kidney laceration (asterisk in a) with perirenal hematoma (arrowhead in a). Active bleeding is demonstrated in the coronal reformatation with MIP (arrow in b). Active bleeding through a small renal artery is also seen in angiography (arrows in c and d).
V – Trauma in Abnormal kidney
Preexisting renal lesions might affect the prognosis and should be suspected in severe lesion after minor trauma.
Renal cysts are the most frequent lesion and they can suffer rupture or bleeding (Figure 11).
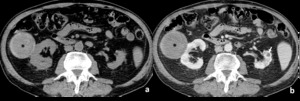
Fig. 11: Renal trauma in a patient with renal cysts.
CT showing an heterogeneous round collection with well defined contours in the right kidney (asterisk in a and b). Contrast-enhanced image (b) shows no renal laceration. Reduced size left kidney with a cyst is also seen (white arrow in b. The lesion in the right kidney is compatible with hemorrhagic cyst. Infected cyst can have a similar appearance due to high proteic content so the clinical history and analytic data are fundamental.
Transplanted kidney (Figure 3) or horseshoe kidneys (Figure 12),
because of their superficial location,
are also prone to any trauma.
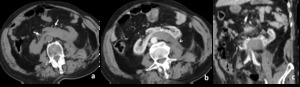
Fig. 12: Patient horseshoe kidney with subcapsular hematoma.
CT of a patient with known horseshoe kidney and abdominal trauma revealing inferior location of both kidneys that are connected in the midline (arrow in a). After contrast injection an hematoma is seen posterior to the left border of the kidney (arrowheads in b and c).
VI – Iatrogenic lesions
Another particularly important group of lesions that deserves to be mentioned are the ones that result from medical intervention.
Biopsies,
but also percutaneous nephrostomy,
partial nephrectomies (Figure 13),
angiography or lithotripsy can result in hematomas,
renal laceration,
vascular injuries,
fistula or pseudoaneurysm formation.
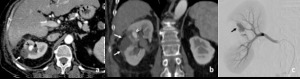
Fig. 13: Patient with subcapsular hematoma and a pseudoaneurysm following partial nephrectomy. Contrast enhanced CT demonstrates the presence of hematoma adjacent to the right renal surgical defect (arrows in a and b) and a hyperattenuating ovoid image nearby (arrowheads in a and b). Angiography demonstrated to be a pseudoaneurysm (black arrow in c).
VII – Complications
Complications after renal trauma are divided in early or late complications,
depending on whether they occur in the first month or after.
In the early period,
urinoma formation and delayed bleeding may occur.
Extravasion of urine due to collecting system laceration (Grades IV or V) may lead to urinoma formation - urine encapsulated or free flowing.
If small urinomas tend be be reabsorbed,
bigger collections or urine may not (Figure 7).
Moreover,
they can infect and lead to abscess formation and urosepsis.
Delayed hemorrhage occurs more commonly in the most severe lesions or conservatively managed penetrating trauma.
Development of hematuria usually 2 to 3 weeks after the traumatic event can be a clue to the occurrence of fistula or pseudoaneurysm (Figure 13).
Late complications,
appearing four weeks after the traumatic event are: hypertension,
hydronephrosis,
calculus or pyelonephritis.
Hypertension secondary to renal trauma can be due to several factors,
as arterial occlusion,
renal compression,
fistula or hematoma formation.
Page kidney refers to hypertension secondary to long standing compression of the renal parenchyma by a subcapsular collection.
Hematoma,
seroma or urinoma enveloping the kidney may lead to compression of the parenchyma and the parenchymal vessels,
decreasing blood flow which will activate the renin-angiotension-aldosterone system and result in maintained hypertension.
The CT will depict the collection involving the kidney,
usually accompanied with parenchymal contour distortion and eventually with delayed nephrogram of the kidney.

 and subcapsular hematoma without laceration(b); Grade II: Perinephric hematoma within the retroperitoneum (c) and small laceration less than 1 cm in depth (d); Grade III: Lacerations greater than 1 cm but without collecting system involvement (e); Grade IV: Renal laceration extending to the medulla and collecting system (f) and segmental infarctions without laceration (g). Injuries of the renal artery or vein with contained hematoma are also included in this category. Grade V: Shattered kidney (h), thrombosis of the renal artery or vein that devascularizes the kidney (i) and ureteropelvic junction avulsion (j).
Bilateral injuries will have one grade upgrade.")
.
CT in a patient reporting blunt trauma demonstrating lack of renal enhancement with irregular border in more than 50% of the right kidney (arrows in a and b). Absence of enhancement is noted in the anterior and peripheral parenchyma. The kidney still mantains its normal contour. These abnormalities are consistent with contusion.")
.
CT in a transplanted kidney patient reporting blunt trauma demonstrating hypeattenuating subcapsular collections in the transplanted kidney, located in the right iliac fossa (arrows in a and b). Contrast-enhancement allows to confirm the presence of a renal collecting compressing the parenchymal contour (arrowhead in b), consistent with subcapsular hematoma.")
.
CT in a patient reporting blunt trauma revealing irregularity of the posterior right renal contour with densification (arrow in a). After contrast enhacement an hematoma envolving the posterior border of the kidney can be seen (arrow in b), along with irregularity of the parenchyma, representing small laceration, inferior to 1 cm in depth (arrowhead in b). The laceration can also be seen adjacent to the hilum in the coronal reformatation(arrowhead in c). Fractures of two vertebra are also demonstrated, findings than commonly occur with these injuries (black arrows in c).")
.
CT in a patient reporting blunt trauma demonstrating hyperattenuating subcapsular collections in both kidneys, previously to contrast administration (white arrows in a). Contrast-enhancement allows to confirm absence of renal laceration. The renal contour is better appreciated in this image and shows bilaterally to be distorted by these collections (black arrows in b) that are well limited peripherally, where they contact the capsule, so one can assume to be a bilateral subcapsular hematomas. In fact, they do not contact renal fasciae (arrowheads in b showing the anterior renal fascia). The same abnormalities can be seen in the coronal image, obtained during the excretory phase, showing no involvement of the collecting system of the right kidney (asterisk in c).
This patient would be categorized as having a grade I renal injury due to subcapsular hematoma, but because of being injury, it increases one grade, being classified as grade II injury.")
.
Patient with blunt trauma in which non-enhancing CT reveals the presence of a hyperdense collection consistent with hematoma (arrows in a). The renal contour is well defined and does no appear to be distorted, suggesting hematoma in the peri-nephric space and not subcapsular hematoma. Contrast-enhanced CT reveals laceration in the posterior pole of the right kidney extending for more than 1 cm (arrows in b). Capsular rupture explains why the blood extends to the perirenal space.")
. Patient with blunt trauma in which non-enhancing CT demonstrates an hyperdense collection involving the right kidney, correponding to a perirenal hematoma (arrows in a). Contrast-enhaced aquisition also reveals a deep laceration in the same kidney, extending to the renal medulla (asterisk in b). Excretory phase aquisition (5 min after contrast administration) allows the detection of urine extravasion from the renal calyx (arrowhead in c) to the collection involving the kidney (arrows in c and d).")
.
Patient with major blunt trauma on the right flank and hematuria showing multiple lacerations of the right kidney, making its contours difficult to distinguish (a and b). These fragments still show normal enhancement, revealing maintained perfusion.")
. A segmental infarction is also seen in the left kidney (arrowhead in a), which shows the classic triangular shape of a non-enhancing renal area, maintaining the normal renal contours. MIP reformatation depicts the branching of the left renal artery at the renal hilum, giving an anterior branch which supplies the only vascularized area of this kidney (arrowhead in c), and a posterior branch that shows complete occlusion.")
. Contrast-enhanced image (b) shows no renal laceration. Reduced size left kidney with a cyst is also seen (white arrow in b. The lesion in the right kidney is compatible with hemorrhagic cyst. Infected cyst can have a similar appearance due to high proteic content so the clinical history and analytic data are fundamental.")
 and a hyperattenuating ovoid image nearby (arrowheads in a and b). Angiography demonstrated to be a pseudoaneurysm (black arrow in c).")
. After contrast injection an hematoma is seen posterior to the left border of the kidney (arrowheads in b and c).")
 with perirenal hematoma (arrowhead in a). Active bleeding is demonstrated in the coronal reformatation with MIP (arrow in b). Active bleeding through a small renal artery is also seen in angiography (arrows in c and d).")